
Five medical breakthroughs in 2024
It's December, and time for a retrospective on some breakthroughs in medical innovation this year.

There are plenty of lists and articles of “medical breakthroughs” out there, but they usually leave me disappointed. Too many focus on early-stage research that might sound exciting but rarely lead to real treatments. These studies can be useful for scientists in the field who know how to interpret the nuances and limitations, but for most people, they’re often misleading or just irrelevant.
I find that frustrating — especially when there are genuine breakthroughs that have reached the final stages of testing that most people still never hear about.
So I want to do it differently. Here I’ve highlighted five medical treatments that have shown high efficacy in (often multiple) phase three randomized controlled trials, which are large, rigorous, and receive much closer independent oversight. I’ve chosen medical treatments whose results were published in 2024.
Because of this criteria, these are just a slice of the important medical advances this year, and only include those that made it through large trials; there are likely a lot more that I’m not aware of, including at earlier stages at research, which can be more difficult to interpret.
As usual, I’ll pay you if you spot an error in this post, aside from minor typos or grammatical errors. Please let me know if you find one, so I can fix it.
1. Lenacapavir: a game changer for HIV prevention
First on this list is the one I’m most excited about.
Lenacapavir is a long-acting antiviral injection for HIV. It was initially approved to treat people with resistant HIV, and recent trials show it’s also highly effective for prevention.
Most HIV prevention methods rely on daily pills, but remembering to take them can be difficult. Stigma and access barriers make it even harder, particularly for people in sub-Saharan Africa, the region most affected by HIV.
Recently, injectable alternatives like cabotegravir, which is taken every two months, have helped. But lenacapavir goes further: a single injection every six months.
The key is its potency and duration. It targets the HIV capsid — the virus’s protein shell — which is a new approach for HIV drugs. And, thanks to clever medicinal chemistry, lenacapavir is stored in fat tissue and slowly released over months. Though its half-life is two weeks, it’s effective in very small quantities, meaning its effects last at least six months.
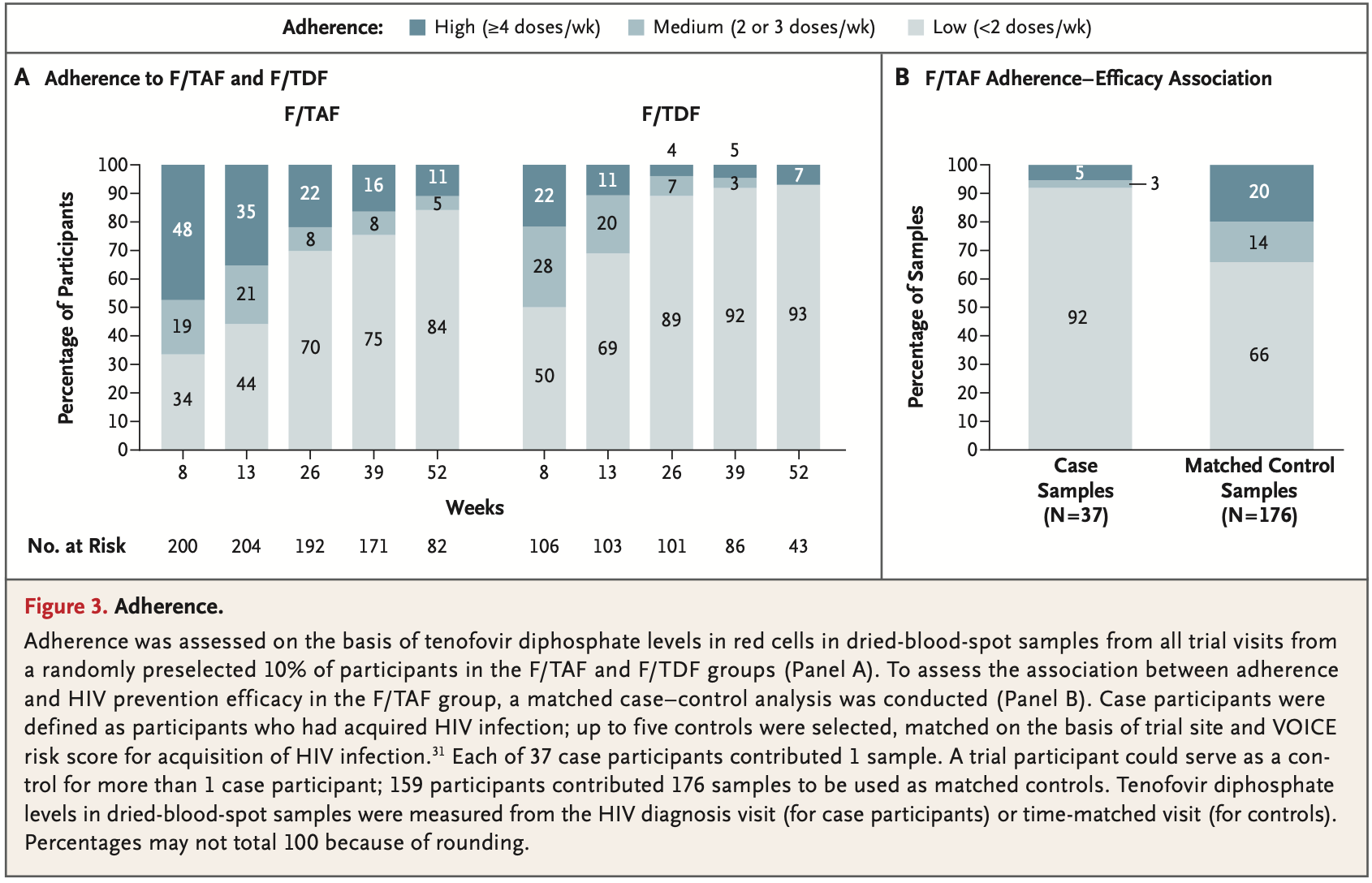
Two recent phase 3 trials have demonstrated its effect as a preventive drug. In the first, with cisgender women in Uganda and South Africa, not a single woman on lenacapavir got HIV — a 96–100% reduction compared to the background risk. And it was over 9 times more effective as tenofovir, Gilead’s daily oral PrEP pill. Here’s the key figure:

In the second trial, involving men and gender-diverse people across six countries, only two people taking lenacapavir out of thousands contracted HIV, an 82–99% reduction in risk compared to the background rate, and again, 9-fold improvement over tenofovir.
It may be surprising that tenofovir, the daily oral pill, appeared ineffective: one major reason is that many people struggle to take it consistently, which can be due to forgetfulness, stigma, or unreliable access, a challenge in the poorest regions.
The chart below shows this: adherence to taking tenofovir declined over time, leaving people less protected. Lenacapavir avoids this problem by requiring just two injections a year, making it much easier to stay protected.
What’s the catch? Trial data shows most people only experienced mild injection site reactions, and had fewer stomach side effects than oral PrEP.
The bigger challenge is scaling it up. Gilead has agreed to allow generic manufacturers in poor countries to sell it so it can be produced and distributed affordably in poorer countries. But for middle- and high-income countries, cost and insurance coverage will be key to access, and health systems will need to find ways to make sure people who need them can actually get their twice-yearly shots.
What’s next? It’s already been in use for a few years as a treatment for people with HIV resistant to other drugs, but now it’s also being tested as a first-line treatment for HIV. A twice-yearly treatment injection, if it succeeds, would also be hugely transformative.
There’s a lot to be excited about, in my view. Innovation like this seriously changes our ability to tackle the global HIV pandemic.
So far, HIV drugs have been able to reduce the severity of HIV and slow its transmission. But preventive drugs have often fallen short because they’re hard to take consistently.
Some countries like the UK are on track to effectively eliminate HIV transmission in the next decade. But infection is still common in poorer countries. Lenacapavir changes that and should raise our expectations for what’s possible, both for the global effort against HIV and the prospect of further innovation.
2. Omalizumab: finally, a step forward in preventive food allergy medication
Omalizumab is a monoclonal antibody drug, given as an injection, which helps people tolerate various food allergens, including peanuts and milk.
It was already approved to treat asthma in 2003 and later, for hives and nasal polyps. In the 2000s, some doctors noticed it was helping their asthma patients with additional food allergies. Unfortunately, insurance typically wouldn’t cover treatment for conditions a drug isn’t directly approved for, so trials were needed to confirm its efficacy against food allergies directly. But those trials hit roadblocks in the 2000s and were stopped, which you can read about in this great article about omalizumab by Sarah Zhang in The Atlantic.
Only recently were larger trials conducted. After positive phase three trial results, the drug was approved this year by the FDA for food allergies.
For people with severe food allergies, exposure to small amounts of allergens can be life-threatening. Current treatments are typically taken after exposure to the allergen, although some people also try “oral immunotherapy” to train the immune system, where people have gradually increased doses of the allergen, but this takes months and can result in severe reactions if it doesn’t work.
On the other hand, omalizumab acts quickly. The drug is injected every 2–4 weeks and blocks “IgE” antibodies, which play a big role in allergic reactions. Blocking them makes the body less sensitive to some allergens.
The new phase three trial, which included people (mostly children and adolescents) with multiple food allergies, showed that omalizumab improved tolerance of small quantities of various food allergens.
As you can see, while 67% of participants in the trial taking omalizumab could tolerate a challenge of 600 mg of peanuts, only 7% taking the placebo could. There was also protection against other food allergies, such as cashews, eggs, and milk:

What’s the catch? Unfortunately, around a third to half of people in the trials still couldn’t tolerate those amounts, even with the drug. You can see this in the same chart above. Also, the amounts of allergens tested were fairly small: ranging from 600 to 1,000 mg.
So, Novartis and Genentech, which manufacture omalizumab, continue to recommend that people taking the drug avoid consuming those foods because it may not provide complete protection. The main benefit is reducing the risk of accidental reactions.
This is still an important advance, especially for young children. It means less fear of a severe allergic reaction to trace amounts, which can be a risk in foods unlabelled or served at restaurants or homes.
I’m excited because I think this signals what’s possible in improving allergy treatment and prevention, and I’m sure there’s still a lot more innovation to come in this area.
What’s next for omalizumab? The results above are only the first part of the phase three trials. Next, researchers will test its longer-term efficacy versus the existing allergy therapy, and third, its protection after introducing food allergens into the diet.
3. Xanomeline-trospium: a new era in schizophrenia treatment
This year, a new antipsychotic drug was approved: Xanomeline-trospium, also known as KarXT (under the brandname Cobenfy).
Unlike many antipsychotics, which target dopamine receptors, this drug targets muscarinic receptors in the brain, but not dopamine receptors, and could reshape future innovation.
, Clozapine (the first atypical antipsychotic), and Xanomeline-trospium (a muscarinic receptor drug) are noted. The timeline also marks significant regulatory milestones, such as the 1962 Drug Efficacy Amendment and the 1970 Controlled Substances Act, which influenced drug development and approval processes. The timeline was produced by Saloni Dattani of Our World in Data.")
The story of xanomeline goes back to the 1990s, when it was originally tested as a treatment for Alzheimer’s disease. During those early trials, something unexpected happened: participants experienced fewer hallucinations, delusions, and episodes of agitation. These symptoms are often seen in schizophrenia.
The results led researchers to test xanomeline as a potential schizophrenia drug. But it led to major side effects, like severe nausea, vomiting, and stomach pain, which ultimately sidelined the drug.
The issue wasn’t with the brain’s muscarinic receptors, which the drug was meant to target. Rather, xanomeline also affected muscarinic receptors outside the brain, especially in the digestive system. To address this, researchers paired xanomeline with another drug called trospium, which doesn’t cross into the brain but blocks muscarinic receptors in other parts of the body. The combination, xanomeline-trospium, allowed xanomeline to work on muscarinic receptors in the brain while trospium minimized its digestive side effects.
With this combination treatment, new clinical trials began.
Three large phase three trials have found that xanomeline-trospium effectively reduces a broad range of schizophrenia symptoms — including what’s called the “positive symptoms” of schizophrenia (e.g. hallucinations and delusions), but also “negative symptoms” (e.g. social withdrawal). You can see this below, and in their pooled results across all trials.

One major difference with previous antipsychotic medications is that xanomeline-trospium lacks movement-related side effects (such as tremors), metabolic changes, and weight-gain that were seen in previous drugs, making them easier to take regularly. See this great post by Nils Wendel for more about it.1
For people with schizophrenia, and their friends and families, this is a really important advance. It’s a step toward more effective, tolerable treatments, and hopefully the beginning of a new generation of antipsychotic medication.
If you’re interested, I recently wrote an article about the history of antipsychotic medication, which I updated after xanomeline-trospium was approved.
Now, research is ongoing on its potential effects on psychosis in Alzheimer’s disease, once again.
4. Tirzepatide: weight loss, diabetes, and more
A list of medical breakthroughs in 2024 wouldn’t be complete without a GLP-1 drug. We often hear about semaglutide, but here I’ll tell you about tirzepatide, a similar drug.
Tirzepatide is a once-weekly injection that helps with weight loss and reduces the risk of diabetes, among other effects.
It works by mimicking two natural hormones, GLP-1 and GIP, which help regulate how the body processes food and sugar. By activating the receptors for these hormones, tirzepatide reduces hunger, increases the feeling of fullness, and improves how the body manages blood sugar.
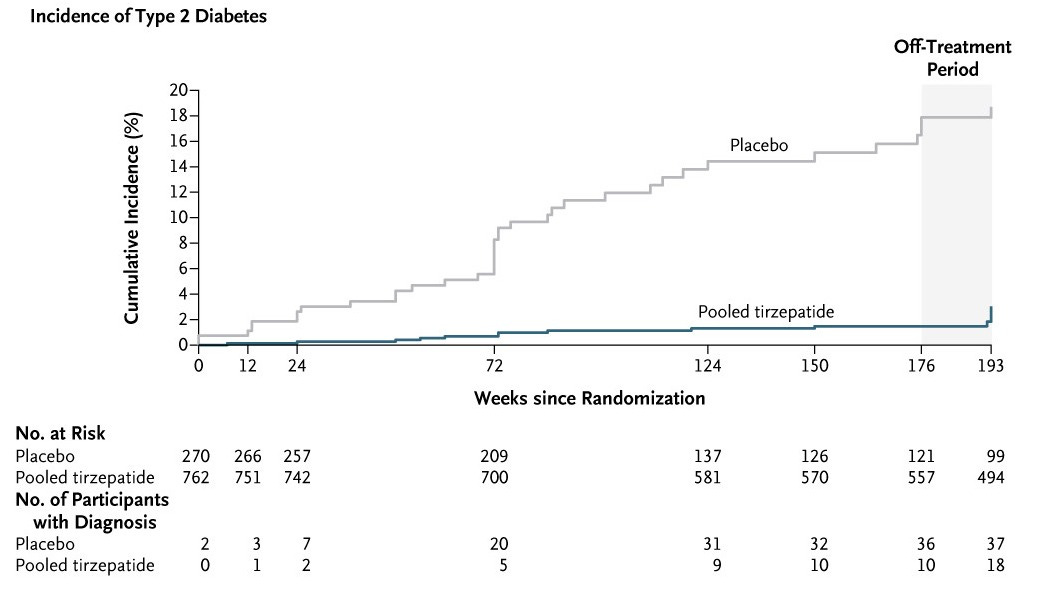
There have been a series of large phase three trials of tirzepatide. In the SURMOUNT-1 trial published last month, people with obesity and pre-diabetes who took tirzepatide had a 90% lower risk of progressing to diabetes, which you can see below.
In the SURMOUNT-2 and SURMOUNT-4 trials, also published this year, tirzepatide helped people lose weight and keep it off.
The SURMOUNT-4 trial (shown below) involved people taking tirzepatide for 36 weeks (9 months), and then being randomized to continue the drug or switch to a placebo. Those on the placebo gradually regained weight over the following year, while those on tirzepatide continued to lose weight — with an average 25% reduction in body weight and waist circumference in under two years.

People with diabetes or obesity are not only affected by the conditions themselves, but also various other health problems, including heart disease, kidney disease, and sometimes sleep problems.
GLP-1 drugs, which were originally approved to treat diabetes, appear to be highly effective against all of the above.2
It’s easy to disbelieve or downplay the importance of these advances, but doing so means ignoring the alternatives and what came before.
Traditional weight-loss methods like bariatric surgery, dieting, and exercise can be effective, but they come with major challenges. Surgery is invasive and costly, while diets and exercise routines are often hard to maintain, especially for people who feel hunger more intensely than you or me.
Many previous attempts to develop obesity medication failed: some had immediate toxic side effects, others increased the risks of psychiatric problems and even suicide, and many simply didn’t work.
Stephan Guyenet wrote a great article about this history for Works in Progress two years ago. Efforts to develop GLP-1 drugs also failed for a long time, until breakthroughs in research finally helped them succeed. With multiple large trials looking at efficacy and safety, I think we can be confident that these new drugs are much safer.
There is a catch though: mild but unpleasant side effects (like nausea, diarrhea, and constipation) are common in people taking GLP-1 drugs, especially at the beginning of treatment.
More importantly, demand for these drugs vastly outstrips supply, given obesity and diabetes are common, and currently only a few manufacturers produce them. It’s going to be important to find ways to scale them up, reduce their prices, and incentivize further innovation.
5. Osimertinib: life extension for people with certain types of lung cancers
Osimertinib is designed for people with EGFR-positive non-small cell lung cancer, which is a form of lung cancer driven by mutations in the EGFR gene. This type of cancer makes up about 10–15% of lung cancer cases in the US, but is much more common in East Asia. It is especially common in people with lung cancer without a history of smoking.
Osimertinib is a small molecule drug that inhibits the EGFR tyrosine kinase protein, which is mutated in certain lung cancers and signals cancer cells to grow and divide.
While it’s already shown clear effectiveness for earlier-stage cancers that can be surgically removed, this latest trial focused on people with advanced lung cancer: specifically, stage 3 non-resectable cancer, meaning surgery is no longer an option. This can be because the tumor has grown near vital organs or spread to nearby tissues or lymph nodes. In these cases, effective treatment options are limited.
Below are results of the LAURA trial, which took place in several countries including the US, India, Japan, Brazil and China.
At the end of the trial, people taking osimertinib were 84% less likely to see their cancer spread or worsen, compared to those on the placebo. Another way to understand these figures is through the time without progression. People on the placebo either died or saw their cancer worsen in an average of 5.6 months. But for those taking osimertinib, this extended to 39 months — almost three extra years.

Osimertinib also reduced the risk of cancer spreading to the brain, which can be a major concern for lung cancer patients. After twelve months, 20% of people on osimertinib developed brain tumors or died, compared to 41% of those who didn’t take it.

Like most cancer drugs, osimertinib can cause side effects. Nausea and vomiting were the most common, but these were mild, and the rate of many other complications was similar in both groups since they are common for people with advanced cancer.
Osimertinib demonstrates that cancer can be held back for years even at a late stage. It’s also another example of precision medicine in cancer treatment: by understanding the genetic mutations that evolve in tumors, scientists can develop more targeted and effective therapies.
Concluding thoughts
For many, these might seem like surprising, one-off advances. In my view, they’re a few striking examples in a continuing stream of medical innovation.
Annual death rates from various conditions, including cancers, cardiovascular diseases, infectious diseases, have declined greatly over the long-run and advances in cancer therapy, cardiovascular medication, antibiotics and vaccines are just a few of the many reasons why. This progress has continued in recent decades, in rich countries. Life expectancy has risen across all ages, across many countries. Records of life expectancy have been broken repeatedly.
In a 2002 paper called “Broken Limits to Life Expectancy”, the great demographers Jim Oeppen and James W. Vaupel describe this progress:
The linear climb of record life expectancy suggests that reductions in mortality should not be seen as a disconnected sequence of unrepeatable revolutions but rather as a regular stream of continuing progress.
And I think they’re right. We’ve continued to see large breakthroughs in medical innovation, and it is interesting and worthwhile to ask how they happened, whether they could’ve happened sooner, how to improve the pace and quality of medical research, and how to make sure that innovation reaches those who need them. After all, this is biology’s century.
Several more specific things also come to mind with these examples.
One is the different ways to work on medical innovation. Medical innovation can mean improvements in efficacy, safety, duration, a wider breadth of effects. It can also mean achieving the same effects with fewer doses, fewer concurrent medications, and so on.
It’s not just the first effective treatment for a condition that’s the breakthrough. “Incremental innovation” can mean the difference between a drug that prevents HIV infections in the long-term versus one that does not reduce the risk in practice, because people don’t take it regularly.
Another takeaway is the importance of various steps in the process of medical innovation:
Basic research has helped understand the triggers of disease and their progression, which helps identify new targets. We see this with lenacapavir (the first-approved HIV antiviral targeting the viral capsid), xanomeline-trospium (the first to target muscarinic receptors in particular instead of dopamine receptors), osimertinib (which targeted particular EGFR-mutated proteins, which research shows drive cancer progression), tirzepatide (developed on the back of understanding the effects of GLP-1 and GIP hormones), and omalizumab (targeting IgE antibodies, which play an important role in allergic reactions).
Medicinal chemistry has helped refine drugs to make them better, safer, and longer-acting. We saw this with lenacapavir (formulated so it would be deposited in fat tissue and slowly released over months), xanomeline-trospium (where the combination helped reduce side effects). But also osimertinib (which can cross the blood-brain barrier, allowing it to reduce cancer spread to the brain); tirzepatide (which is a synthetic protein that acts on both GLP-1 and GIP receptors); and omalizumab (where the antibody structure’s gives it high specificity and safety for targeting on IgE antibodies).
Repurposing existing drugs can be transformative. Omalizumab (originally for asthma) and xanomeline (originally tested for Alzheimer’s) were successfully repurposed for new uses, highlighting that breakthroughs don’t always require brand-new molecules — sometimes just a new application. Researchers know this, of course, and occasionally, the process of screening existing drugs leads to new repurposing.
Sometimes it takes many years for drugs to make it to the market. Omalizumab (originally developed in the 1990s and approved in 2003) and xanomeline (also developed in the 1990s) are the clearest examples of this, though fortunately there were shorter timelines between development and approval for the other drugs. The history of antipsychotic medication also includes another pivotal example: clozapine, which was developed in the 1950s but first approved in the US in… 1990. Clozapine’s story is important because it inspired much more innovation in the field of antipsychotic medication; I’ve written about why the process took so long in an earlier article.
Timelines are often long especially for neglected conditions, where there’s often little financial incentive for pharmaceutical innovation; and for rare and sporadic diseases, where it’s difficult to recruit enough participants for trials or reliably test drugs’ effects. This doesn’t need to be the case, and there may be new pathways and incentives to accelerate their research.
I’ll end there, except to apologize for the long delay since my last post (eight months ago, yikes!) There’s unfortunately no one to blame but myself: I had several half-written drafts that I scrapped, got caught up in other work and hobbies on the weekends (which is when I usually write this), and found it hard to carve out the time to write.
But now I plan to write this regularly again, hopefully every week.
As always, I hope you enjoyed reading this. If you haven’t already, I hope you subscribe and share it with your friends! If this is your first time here, I recommend reading the About page.
This Substack is free, I have no plans to monetize it, and I’ll pay you if you spot any errors in this post and let me know. (Minor typos and grammatical errors excluded.) If that’s not a great deal, I don’t know what is.
See you next time! :)
– Saloni
On 9 Dec 2024, I updated these paragraphs to remove the statement that many previous antipsychotic drugs don’t reduce “negative” symptoms, as it was more common than I realized. I also added a brief paragraph to say that the trials showed a lack of various motor and metabolic side effects with xanomeline-trospium that were seen in previous drugs. Thanks to Nils Wendel for pointing these out in a comment!
See the following trials on semaglutide and cardiovascular disease, kidney disease, and tirzepatide on cardiovascular disease and sleep apnea.
Hi! Psychiatrist here. Great writeup, I'm always happy to learn about breakthroughs in other specialties that I've lost touch with! It's especially nice to see long acting injectable medications develop outside of psychiatry.
I just wanted to make a couple comments about Xanomeline-Trospium to add nuance to the conversation.
In my view, the lack of side-effects is where the drug really shines - the antidopaminergics (i.e. previous antipsychotics) have a slew of movement and metabolic side effects that Xanomeline just doesn't. I expect it to become a first line treatment once it's off patent.
I think that the narrative regarding improvement of negative symptoms with xanomeline has been a bit misleading and frankly oversold. First, I don't think it's quite right to say that the antidopaminergics don't treat negative symptoms. They absolutely do, just not as well as the positive symptoms. Consider risperidone's effect size on positive symptoms (d = -0.61) vs. negative symptoms (d = -0.37). (Source: Huhn et al., The Lancet, Sept. 2019)
This isn't substantially different from the effect size on negative symptoms found in EMERGENT-2 (d = -0.40), and I don't think is substantially better than most antidopaminergics, which are somewhere around (d = -0.35). I'd also note that EMERGENT-3 did not show a significant improvement in negative scores at their endpoint.
My guess is that xanomeline-trospium will (unfortunately) look much like the other antipsychotics in terms of efficacy on negative symptoms as more data comes out, though I hope to be proven wrong!
Omalizumab is also used to treat chronic urticaria (at least in France).
It has been a game changer for me. I used to have urticaria every day (itching and pimples everywhere) but since I've been injecting myself with Omalizumab once a month, I've had nothing.