
#18: A slice of great things you missed this year
This post: A brain cancer breakthrough, defeating dengue, women's employment, rabies elimination, personality and age, giant virus-like particles, and more.

This is my eighteenth post of Scientific Discovery, a newsletter where I’ll share great new scientific research that you may have missed. Check out the About page if you’re interested in why I’m writing this.
Every so often on this blog, I put together great research that I feel should be read more widely.
This blog is called Scientific Discovery – but scientific discovery is just the beginning. We not only need to understand the world and discover ways to make progress, but also find out how to scale them up so they can make a real difference to people’s lives.
In this post, I’ll cover research on: a brain cancer breakthrough, controlling mosquito diseases with bacteria, rabies elimination, women’s employment, personality and age, and more. This post is too long for email. I hope you enjoy it! If you spot a mistake, let me know and you could earn a reward.
A brain cancer breakthrough
Phase III trial results: Vorasidenib in IDH1- or IDH2-mutant low-grade glioma (Ingo Mellinghoff et al., 2023)
Brain cancers aren’t the most common cancers, but they tend to be the most devastating. Brain cancer patients die about 20 years earlier than they would otherwise, on average.1
This is about a new drug that can change that. What’s even more hopeful is that, because of the way it was developed, it’s likely to be just one of many drugs in this new category.
Let me give you some context. This drug works against brain tumours from glial cells – these are cells that have many functions, including supporting neurons. Their tumours are called gliomas.
There are about 140,000 patients living with gliomas in the United States.2 This makes them one of the most common brain cancers; they’re about a quarter of all brain cancers. Patients are diagnosed with low-grade gliomas at the age of 41 on average, and then have an average survival time of around 7 years.
So far, treatments for child patients with gliomas have been quite effective. But for adults, who have different types of gliomas, the situation has been pretty dire.
Radiation and chemotherapies aren’t so effective. Brain surgery is risky, especially if the tumour is in a critical part of the brain. So, at early stages of the cancer, many patients ‘wait and watch’ – with chemotherapy and regular MRI scans to see when it worsens.
This new oral drug, called vorasidenib, is one in a new category that can change that.

How does it work? You may know that tumours develop from uncontrolled growth. This happens through many pathways – one way is by altering their metabolism, which lets them multiply and grow quickly.
This new drug blocks two key metabolic enzymes, IDH1 and IDH2, which help them do that. Their tumours become somewhat dependent on this new metabolic pathway. About 80% of glioma patients3 have a mutation in these enzymes – and it turns out, so do a share of patients with a range of other cancers – which suggests this drug could be widely useful.
In this phase 3 trial, over 300 patients with recurrent glioma and mutations in IDH1 or IDH2 were given vorasidenib or a placebo.
The chart above shows that those who received the drug survived without a progression in their cancer for a median of 28 months, versus 11 months in the placebo group, which is 2–3x as long. Their side effects were mostly minor, but some patients developed liver toxicity.
Why am I excited about this? Although brain cancers still remain serious, this is a major step forward in our understanding and ability to treat them. The drug is now under fast-track for approval by the FDA. Another point that’s hopeful is that it’s one of several new drugs. The reason behind this is that scientists know what makes it work and why – it wasn’t discovered by chance, but through ‘rational drug design’.
Mutations in the IDH1 and IDH2 metabolic enzymes had been identified in gliomas over a decade ago through genetic sequencing. Since then, multiple IDH-inhibitor drugs have been developed, using structural imaging techniques and medical chemistry. The other drugs have also had promising clinical trials, but vorasidenib seems particularly effective because it’s able to target both enzymes.

The list of big cancer breakthroughs in modern history is pretty long – tamoxifen, cisplatin, vinblastine, imatinib, trastuzumab, rituximab, ipilumumab and methotrexate are just some of the biggest, and hopefully this will join the list. Each of these has an important story, and I’d like to write about them more. [For now I’ve linked to brief histories of each in case you’re interested.] There are also the new ‘CAR T-cell therapies’, which I hope to have time to write about later as well.
At the same time, cancer treatment still has a long way to go. It’s not just efficacy that we care about, but how to make drugs safer and easier to take in the long-term, without toxic side effects. This has been an under-appreciated part of the history of medical progress, and it continues to matter.
But another reason I find this exciting is because it’s an example of the modern revolution in biotech, or what people call ‘the century of biology.’ Biotech advances are rippling through the field, and it’s crucial that we streamline the process of clinical trials and regulation to help draw them out and scale them up, so everyone can benefit from them.
Defeating dengue with Wolbachia
In more biotech news, let’s talk about a way to stop mosquitoes from spreading disease.
Maybe you’ve vaguely heard of Wolbachia – it’s a species of bacteria that blocks some mosquitoes from spreading some viruses to us, but causes negligible harm to us or the environment.
It came back to my attention because at a recent conference, researchers presented their findings that Wolbachia programs reduced dengue incidence by 94–97% in areas where they were highly established in three Colombian cities4, in the biggest field trials so far.
That’s huge if true, but since those results haven’t been published yet (here’s the original plan for the study), I decided to look into previous papers on the topic. Here’s a little summary.
Briefly, pilot programs have been quite effective so far – some have now been running for over a decade, and they shouldn’t be seen as a far-fetched experimental idea.
How does it work? To begin with, researchers insert Wolbachia bacteria into the eggs of female mosquitoes, with microscopic needles. The mosquitoes then pass it onto their offspring – who maintain the bacteria in their reproductive cells throughout their lives.
In the most common approach, Wolbachia blocks many mosquitoes from carrying dengue virus (and some other viruses), but it doesn’t shorten the mosquitoes’ lives.5 This helps them lay many infected eggs and propagate and replace the existing population quickly.
To top it off, male Wolbachia-infected mosquitoes can’t produce eggs with female mosquitoes that aren’t infected – so Wolbachia-mosquitoes have a reproductive advantage.6 All this gradually increases the share of mosquitoes that are infected with Wolbachia, and reduces the share of mosquitoes that carry dengue.

Diagram to explain the Wolbachia method to reduce diseases like dengue. Source: World Mosquito Program. Getting to this point took lots of scientific research. Here’s a highly recommended article about it by Scott O’Neill, one of the leading scientists and founder of the ‘World Mosquito Program’, which helps run many Wolbachia efforts.7
Where has it been tried, and for which diseases? By now, Wolbachia has been used to control mosquito-borne diseases in regional pilot projects in several countries: Australia, Indonesia, Brazil, Colombia, French Polynesia, Vietnam and more.
So far, it’s been used for Aedes mosquitoes, which spread multiple diseases to us: dengue, Zika, chikungunya, and yellow fever.
In case you didn’t know, dengue and chikungunya are debilitating diseases of joint pain that often last several weeks or months. Zika is a risk to pregnant women and fetuses. Yellow fever can cause severe liver damage, and jaundice.
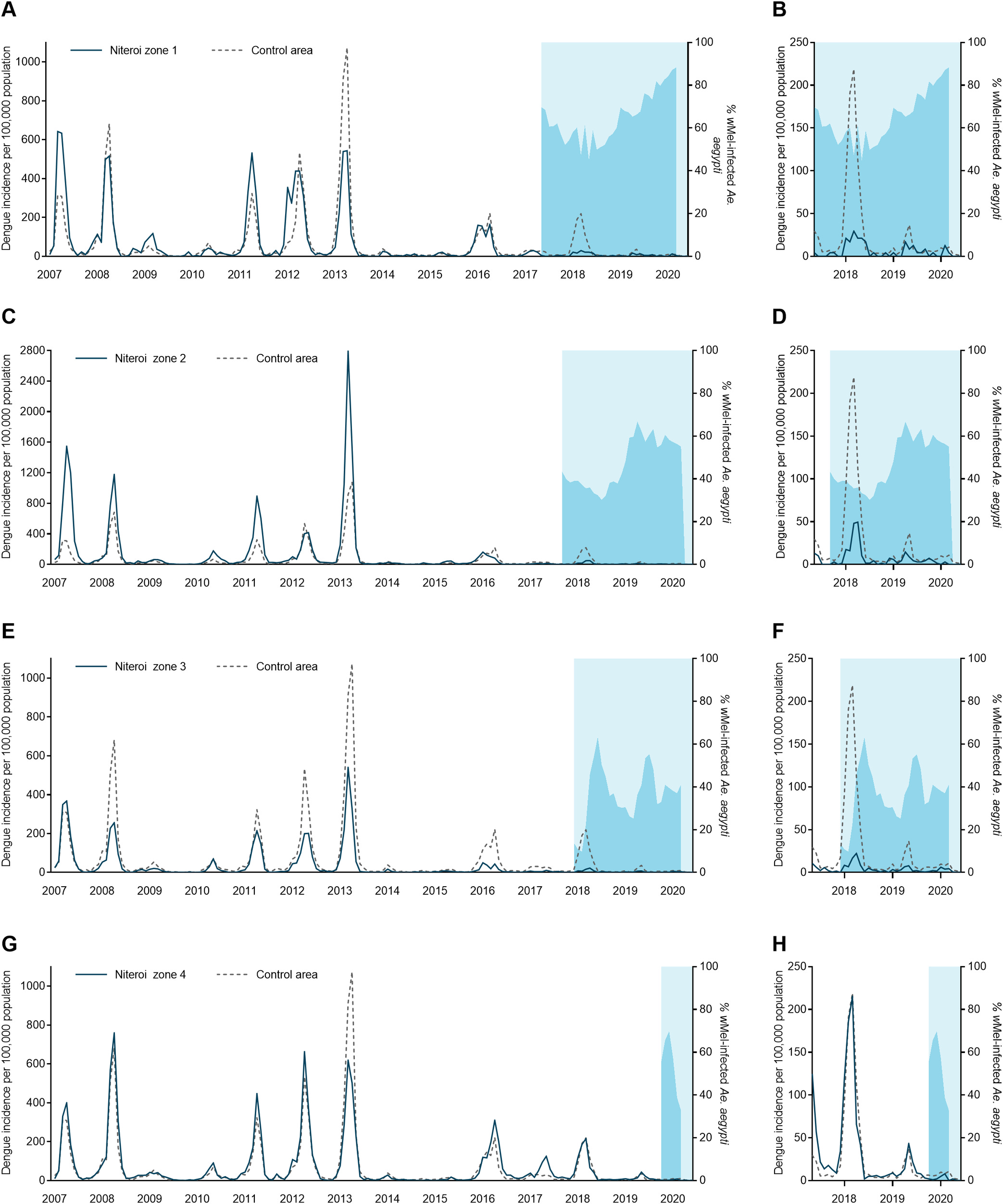
How effective is it? Previous Wolbachia projects have been fairly effective at reducing dengue. A recent cluster-randomized controlled trial found that it reduced dengue incidence by around 77% in Yogyakarta, Indonesia8; another recent field trial in Niterói, Brazil led to a 69% reduction (shown below). The earliest program led to a 96% reduction in dengue in Queensland, over the span of a decade.
These diseases are highly seasonal, so there’s sometimes uncertainty around precisely how effective it is, especially when looking at shorter timespans – but the data overall suggests it’s fairly effective against dengue.
Wolbachia efforts aren’t as effective for other diseases (chikungunya, Zika, yellow fever) yet, but still look effective. This may change with more research.

A time-series chart showing the rates of dengue before and after the program began in Niterói, Brazil. This is compared between the treated areas (solid lines) and control areas (dashed lines). Light blue shows when the program began. Dark blue shaded areas show the share of wild Aedes aegypti mosquitoes that now carry Wolbachia. Source: Effectiveness of Wolbachia-infected mosquito deployments in reducing the incidence of dengue and other Aedes-borne diseases in Niterói, Brazil: A quasi-experimental study (Sofia B. Pinto, et al., 2021)
These programs have a big upfront cost, to prepare Wolbachia-infected mosquitoes. But in urban areas where dengue is common, they still seem very cost-effective, and the benefits grow over time as more dengue cases are prevented.9
Wolbachia programs could lead to elimination of dengue in (some? many?) countries, if rolled out widely. In some pilot program regions, such as Queensland, Australia for example, it already has.
At intermediate levels of Wolbachia efficacy, it’s estimated that programs if rolled out widely could reduce global dengue incidence by at least 70%. This is according to modelling studies which find that programs have been effective enough to reduce the R number below 1.
But this depends on the baseline prevalence of dengue, the implementation and monitoring, which could be difficult in some areas.

One worry you might have is: could resistance evolve somehow?
Maybe Aedes mosquitoes could become resistant to Wolbachia? Or maybe dengue viruses could become resistant to Wolbachia?
The first seems unlikely – Wolbachia has remained stable at high frequency in Aedes mosquitoes for over a decade in Queensland and in Malaysia, which had the earliest programs. They’re also fairly pervasive in the insect world, likely because of their reproductive effects.
The second is less clear – dengue viruses evolve quickly, have many strains, and Wolbachia doesn’t give mosquitoes complete protection from them. A recent study reviews the evidence on this. This situation could change – but Wolbachia’s efficacy could be improved scientifically too.
A crucial part is to prepare with more research and monitoring, even after the programs have been successful. Overall though, it looks like this should be scaled up more widely, and I’m pleasantly surprised by how effective it seems to be.
The summer drop in female employment
Working paper: The summer drop in female employment (Brendan M Price & Melanie Wasserman, 2023)
Let’s move onto something completely different, spurred by this year’s Nobel prize to Claudia Goldin, for her work on gender differences in the labour market.
I’ll talk about a new study about women’s employment and how it drops in the summer – the charts and findings are very interesting.
The authors look at this topic with data from the US Current Population Survey, which is a monthly survey of around 60,000 households, conducted by the Bureau of Labor Statistics. Below is a summary of what they find.

The authors find that women’s formal work10 drops during summers, both in terms of employment and job-seeking. And even among women who continue to work, their working hours decline – much more than men’s.
In total, women’s hours-worked shrink by around 9.8% from May to July (considering both the employed and unemployed), which is more than double the decline seen in men.
Why does this happen? The paper argues that it’s because they’re more likely to take time off to care for children on their summer breaks. They find many lines of evidence that support this idea:
The size of the decline is largest among women with school-aged children, and women without children don’t experience a decline. Also, the timing of the decline matches school closures; and the overall decline is almost fully accounted for by the share of women with children who say they’re taking care of house or family, in the surveys.
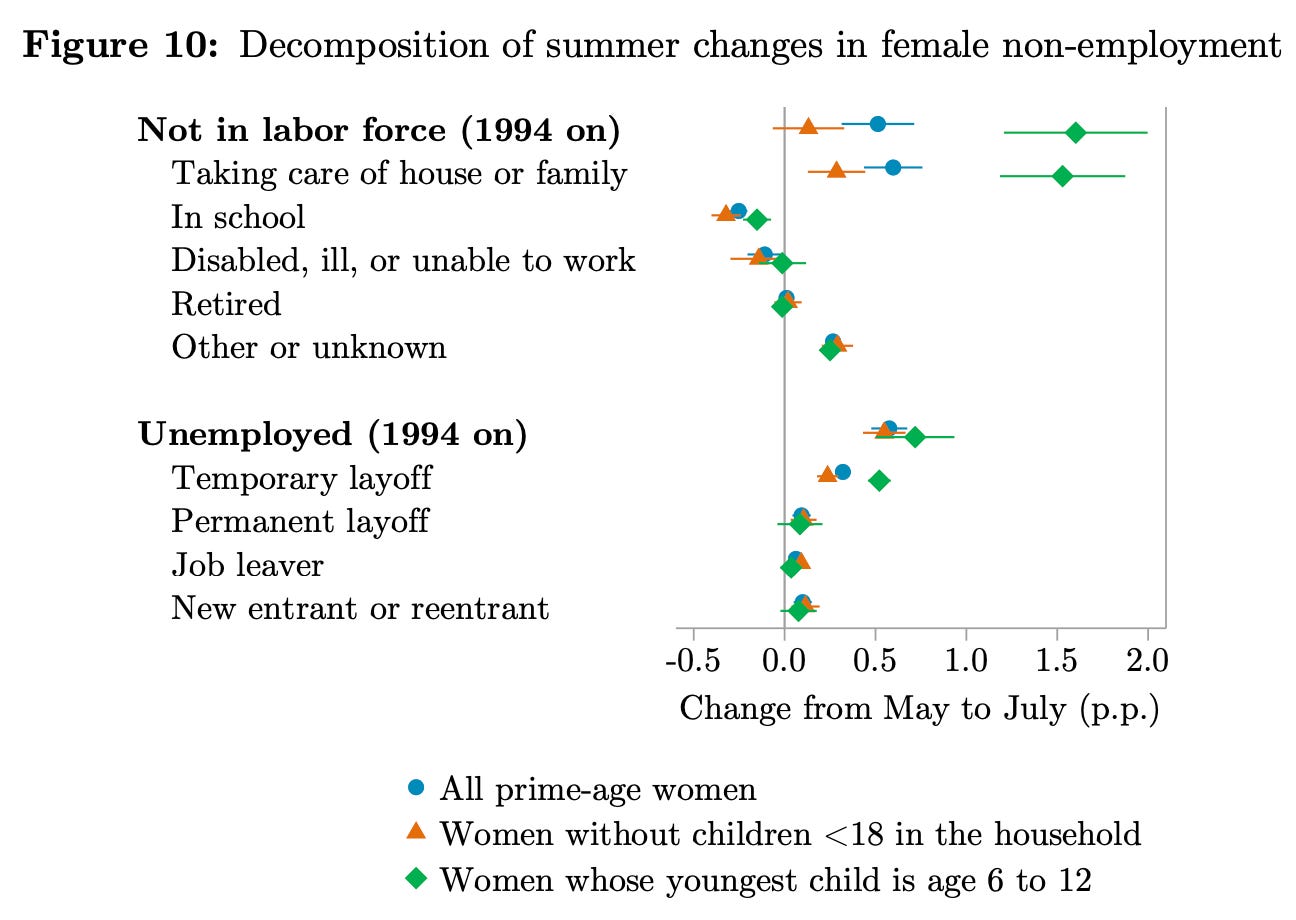
Another interesting finding is that women are more likely to work in education if they have a young, school-aged child (shown in the chart below). This is presumably because it’s much easier to match children’s time off school.
Through this, I also learnt a new statistic: in total, around 13% of working women in the US are in the education sector.

More
Do people become more conservative as they get older?
Older people are more likely to agree with conservative ideas, and say they’re conservative. But if you track a cohort of people over time, at least in the US, they tend to become more liberal as they grow older. How can these both be true?
Allen Downey explains this seeming-paradox. If people become more liberal with age, but younger cohorts are even more liberal than them, then older people appear more conservative as they age, relatively speaking.

This chart shows the level of conservative responses to political questions in the General Social Survey (GSS) in different birth cohorts, as they aged. You can also see that younger cohorts are less conservative. It comes from an interactive explainer that explains the seeming-paradox in age and being conservative. Source: Brilliant.org, based on Allen Downey’s book.
How do our personalities change with age? (Ingo S. Seifert, Julia M. Rohrer, and Stefan C. Schmukle, 2023)
To answer this question, it’s important to distinguish generational differences from changes with age. In this study, researchers looked data from cohorts as they grew older (in three datasets – from Germany, Australia and the Netherlands).
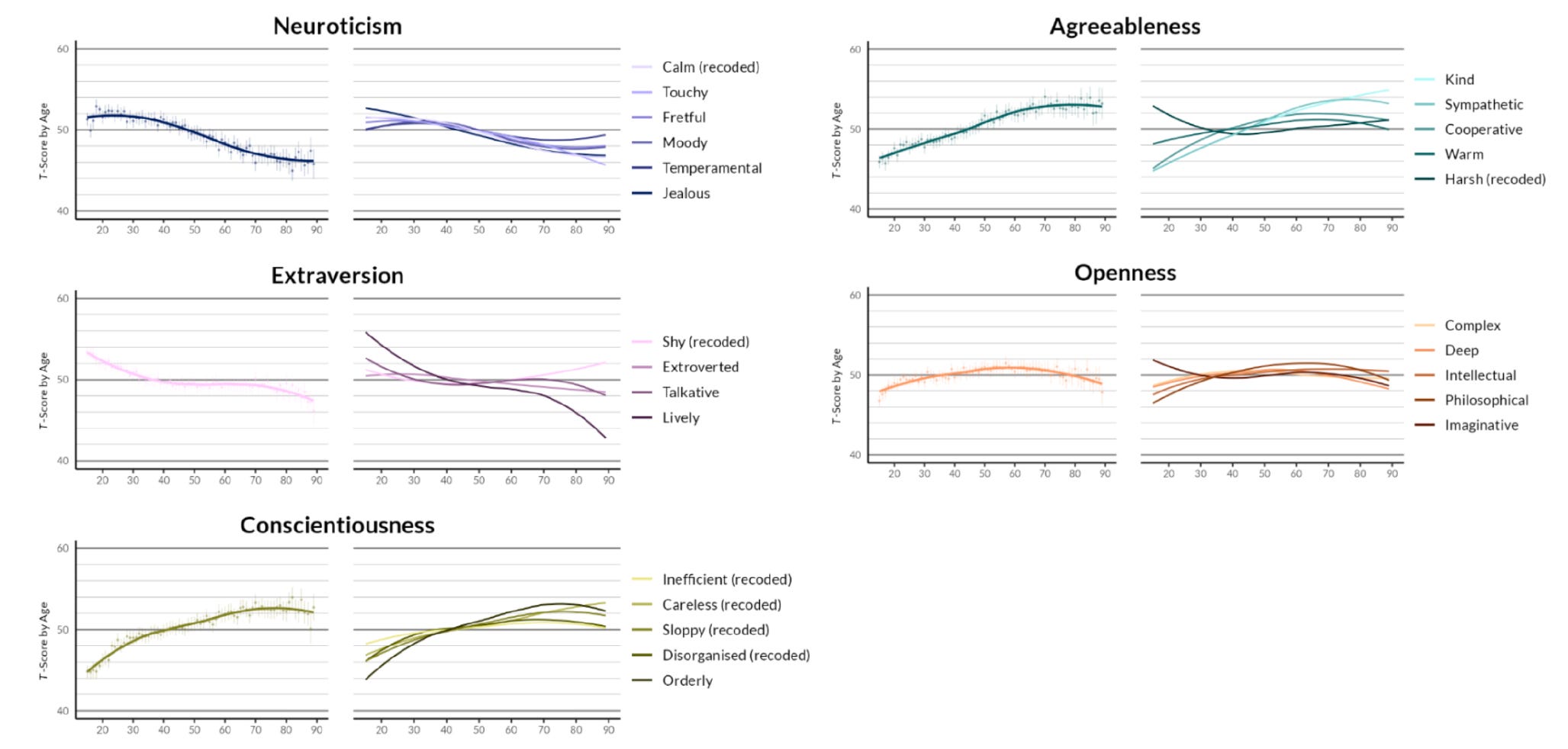
With this, they found some consistent changes – across all three datasets, people became more ‘conscientious’ and ‘agreeable’ until middle-age, and less ‘neurotic’ across their lifespans.
But, each of these traits is an average of answers to multiple questions (for example, agreeableness was measured with questions about kindness, sympathy, cooperation, warmth, and harshness). And as you can see below, the individual answers often showed different trajectories.

Human rabies was eliminated in Goa, India. (Andy Gibson et al., 2022)
Here are a few points to put this in context:
India is estimated to have the largest burden of rabies worldwide, making up perhaps a third of all rabies deaths globally.11 This is likely the result of a large population as well as a large population of free-roaming dogs, poverty, poor understanding of rabies, and a lack of coordinated strategy that was used here.
Rabies is near uniformly fatal in people if they aren’t vaccinated (vaccinations are typically given post-bite). But prompt vaccination is very effective, making fatalities rare. (This is an amazing story in its own right.)
At the same time, vaccinating humans has little impact on the spread of rabies. Rather, it’s dogs and other animals who are reservoirs for the disease, and happen to spread it to us, which is why animal vaccination is effective.
Animals can be vaccinated through injection or oral bait (which have sometimes been dropped from helicopters across European forests), and it’s estimated that only around 45% of all dogs need to be vaccinated to achieve elimination.12
So how was it eliminated in Goa? Between 2013 and 2019, this program involved:
Door-to-door (DD) vaccination (for confined dogs) and capture-vaccinate-release (CVR) (for free-roaming dogs) through GPS coordination, along with vaccination surveys;
School-based education to almost 700,000 children about how to avoid dog bites, what to do if bitten, and the importance of dog vaccination;
A widely-publicized rabies hotline, to help people request vaccinations or report sick or injured dogs (with or without rabies).
By the end, there was a 92% reduction in monthly canine rabies cases, and human rabies deaths had been shrunk to zero.

Giant virus-like particles in soil (Matthias G. Fischer, Ulrike Mersdorf, Jeffrey L. Blanchard, 2023)
You might know that the first virus (the tobacco mosaic virus) was described in the 1870s. For decades after that, viruses were described in terms of what they were not – they couldn’t be seen, they couldn’t be retained by filters, they couldn’t replicate without cells – until we finally found out what they were. (The first time viruses were seen was in the 1930s, using electron microscopes, which were new at the time and apparently called ‘übermikroskope’.)
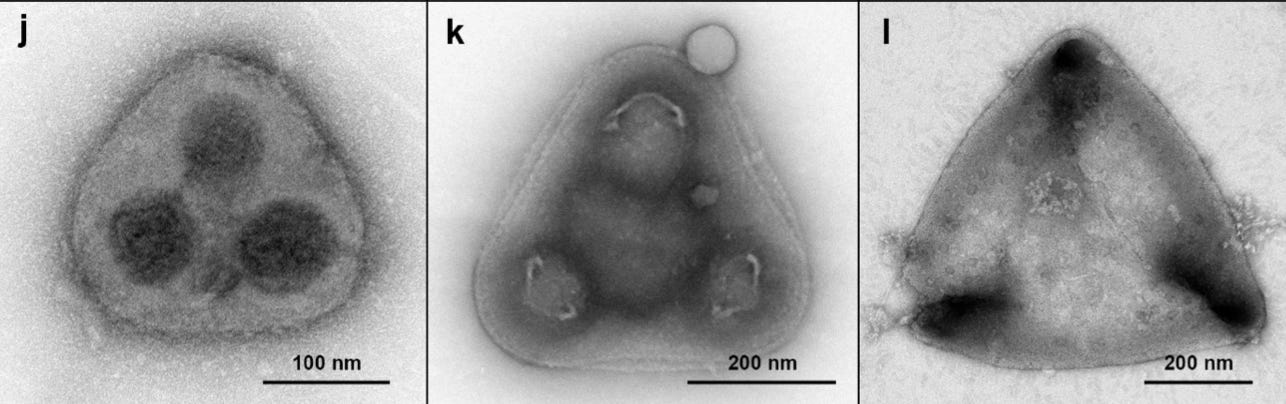
But did you know that some viruses are so big that they can be seen with regular microscopes? These ‘giant’ viruses are still fairly small – only around 1 micro-metre (i.e. 1/1,000th of 1mm) – but they’ve changed our understanding of viruses.13
This new study is about a range of giant particles in soil that look like viruses (but may or may not be viruses). Here are some cool, spooky photos of them.


I actually had a heap of other papers I still wanted to share, but I’ll stop there! Enough fun facts already.
Even more
Here are some links from around the web that I enjoyed recently:
‘How to save twenty million lives’ – a very inspiring written interview with Dr. Mark Dybul, who led PEPFAR: a program that scaled up AIDS treatment in Africa and saved millions.
A long-form podcast interview with Katalin Karikó, this year’s Nobel laureate in medicine for her work on mRNA. I hadn’t known much about her life before listening to it, and I found the episode very honest and moving.
The Arctic Permafrost Atlas – a freely available book with loads of beautiful maps and diagrams that explain permafrost (pdf link, which is 236 Mb).

A little preview from the book. The actual book has probably over a hundred maps and charts. Source: The Arctic Permafrost Atlas A podcast episode on the destruction of Pompeii by Mount Vesuvius’ eruption in 79 AD. I recently visited Pompeii and Mount Vesuvius and listened to lots of great podcast episodes about their history while I was there – this was the best one.
The Invention of Surgery, a book by David Schneider. Many surgeries we consider minor now were once very risky, if not fatal. This is a nice book that chronicles how that happened, & the people who pioneered surgical advances.
Niko McCarty’s guide to synthetic biology – full of links and reading to introduce you to different parts of synthetic bio.
‘Large language models, explained with a minimum of math and jargon’ – by Timothy B Lee and Sean Trott. Exactly what it says!

What I’ve been up to
I was on a podcast!
I recorded a great fun, 3 hour long conversation with Fin Moorhouse and Luca Righetti on Hear This Idea. We talked about the history of malaria, the incredibly long (& frustrating) journey to a malaria vaccine, missing data & more. Listen here.
I discovered a mistake in an earlier post I wrote.
In post #15 ‘What does it mean when fewer people die’, I inaccurately described the ‘survivorship age’ from a study. For example, the sentence: ‘It shows that women in France who died at the age of 90 in 1900 were in the top 1% of survivors in their cohort.’ was inaccurate. Rather, it should have said something like: ‘It shows that among those born in 1900, women in France who die at the age of 90 would be in the top 1% of survivors.’ That’s quite a different interpretation, and it also affected other parts of that section. I’ve now corrected it.
I found this experience annoying for several reasons: I had re-read the study several times to make sure I was describing it accurately (it was ambiguous); it would have been easy to correct quickly had I known; and people with more experience in demography should have caught it easily, for methodological reasons – but it wasn’t pointed out to me, and only came to mind because I was working on a related topic once again.
So I’ve set up a reward system for people to point out mistakes I’ve made.
You can earn £5, £15, or £40 for letting me know about a mistake I’ve made, including in this post. There are more details on my About page here. I hope this also motivates me to spend even more time fact-checking.
I wrote some articles:
How are causes of death registered around the world? – everything you wanted to know about causes of death and how they’re determined, and why this data is often missing in poor countries.
Why death tolls from different risk factors can’t be simply ‘added up’. This point is frequently overlooked, which means people don’t realise that the same deaths can often be prevented in multiple ways.
I made some pretty charts, like this one:
I’ve been eating a lot of gelato, as usual.

Me with two scoops of gelato (they were fig and pistachio flavoured). I didn’t do anything interesting for Halloween this year, but that’s because I no longer have my favourite costume.


And that’s all for now. I hope you enjoyed this, learnt something new and subscribed if you haven’t already.
This newsletter is completely free, I’ve turned off subscription pop-ups, and I guess I’m now offering rewards to readers too – if you let me know about mistakes I’ve made. So why not share it with your friends too, and ‘earn while you learn’?
See you next time!
– Saloni
This statistic comes from the US CDC, but it may vary elsewhere – for example, in countries where even modest treatments and surgery aren’t available, the number of life years lost could be higher.
This statistic comes from data from 2016 to 2020. Gliomas have an incidence rate of around 5 per 100,000 people per year, according to national registry data from Finland and other sources.
This comes from a 2009 study of around 400 brain tumour patients, but it’s not clear to me whether newer data is available.
Corrected 4 Nov 2023. This originally said the programs reduced dengue incidence by 94-97% across three Colombian cities. However, the linked article referred specifically to the decline in neighbourhoods where Wolbachia was highly established. Iʼve now corrected this to reflect that.
Some countries like Singapore use a different approach – trying to suppress mosquito populations overall: Wolbachia-infected males mate with wild females, and the resulting eggs do not hatch. In this post, I’ve focused on the disease-blocking approach, which has been more commonly used.
This is due to ‘cytoplasmic incompatibility’: Wolbachia changes the sperm of infected males, which leads to mismatches during egg fertilization. Uninfected eggs can’t correct these mismatches, resulting in embryonic lethality, while Wolbachia-infected eggs can, which allows them to mature successfully.
Or try this review or this more-recent one for a more technical explanation.
I lean towards thinking this is an underestimate of the efficacy, because the prevalence of Wolbachia also began to rise in the control areas, due to ‘contamination’. In this case, contamination refers to the spread of Wolbachia-infected mosquitoes from the treated areas into the control areas, especially at the edges of regions. (You can find the paper here.)
‘Formal work’ here refers to regulated, paid employment with legal protections and benefits. Meanwhile informal work – e.g. caregiving and housework, which are disproportionately done by women – lacks such formalities and often doesn't provide stable income or benefits. In the rest of this section, I’m referring to formal work.
Like other neglected tropical diseases, there’s uncertainty around these estimates. This tends to be because of poor or dysfunctional death registration in poor countries. I’ve written about this recently here.
The estimate in the study (which used data from rural Tanzania) ranges between 20–45% vaccination coverage; I’ve put down the upper limit here for simplicity, as a conservative estimate. Since there is a large ‘turnover’ of dogs each year (births, deaths, migrations) in Tanzania, the authors estimated that around 70% of dogs should be vaccinated each year in that region, for example, to maintain a total vaccination coverage of 20–45%. (This is likely to vary in other regions.)
You might be wondering how the first virus was discovered before viruses were even seen. Scientists had previously discovered infectious material that was so small that it couldn’t be retained by tiny filters; and decided to call the material virus. In fact, for a while in the early 20th century, there was some debate around whether viruses were particles or fluid – the case was closed when they were seen under electron microscopes in the 1930s (spoiler: they were particles).
Anyway, fast forward to the discovery of mimiviruses in the 1990s, which were so big they were originally misidentified as bacteria. This led to new understanding that the typical ‘filtration’ method to identify viruses had excluded a range of viruses.
You do awesome work!
A great read! Thanks for the work you do for humanity.